


Duchenne Muscular Dystrophy: Overview and Epidemiology
Written by Margaret Anne Rockwood | Last updated June 2nd, 2026
 Medically reviewed by Daniel Guillen, MD
Medically reviewed by Daniel Guillen, MD
Duchenne Muscular Dystrophy: Overview and Epidemiology
Muscular dystrophy (MD) comprises a heterogeneous group of inherited neuromuscular disorders. These are all characterized by progressive myofiber degeneration, resulting in skeletal weakness and varying degrees of functional impairment. They arise from genetic mutations that affect proteins essential for muscle structure, stability, and function.
Although individually rare, muscular dystrophies collectively represent a significant cause of inherited neuromuscular disease worldwide, causing chronic disability, cardiopulmonary complications, and reduced life expectancy in affected individuals.
In Duchenne Muscular Dystrophy (DMD) in particular, new treatments on the leading edge of molecular science are showing promise in slowing cardiac muscle degeneration, a major precursor of rapid decline. Thanks to accelerated approval pathways, these therapies are making their way into the clinician’s hands more quickly, which is critical for patients experiencing a progressive, irreversible disease.
Muscular Dystrophies at Large
The underlying pathology in most muscular dystrophies involves mutations affecting proteins that stabilize the sarcolemma, the outer covering of a muscle cell that helps it receive and transmit signals needed for contraction, maintain cytoskeletal integrity, and regulate muscle fiber function. Over time, affected muscle fibers undergo necrosis and are replaced by adipose and fibrotic tissue, leading to progressive weakness and contractures.
More than 30 genetically distinct muscular dystrophies have been described. They are classified based on clinical phenotype, pattern of inheritance, age of onset, and the specific gene involved. Nine of the most clinically significant forms comprise 90–95% of all cases.
These include Duchenne Muscular Dystrophy (DMD), Becker Muscular Dystrophy (BMD), Limb-Girdle Muscular Dystrophies (LGMD), Facioscapulohumeral Muscular Dystrophy (FSHD), Myotonic Dystrophy (DM), Congenital Muscular Dystrophies (CMD), and Emery–Dreifuss Muscular Dystrophy (EDMD).
- X-linked disorders (e.g., Duchenne and Becker muscular dystrophy) predominantly affect males. Approximately 65–70% of cases are inherited from a carrier mother, while 30–35% arise from de novo mutations.
- Autosomal dominant forms. (e.g., facioscapulohumeral and myotonic dystrophy) In FSHD, reduced penetrance and variable expressivity affects phenotype; in myotonic and other trinucleotide repeat disorders, vertical transmission is common, with worsening disease across multiple generations.
Autosomal recessive forms (including many limb-girdle muscular dystrophy subtypes and congenital muscular dystrophies) are more common in populations with higher rates of consanguinity. Since the disease manifests only when both parents carry and transmit pathogenic variants, these forms are usually found as isolated cases without prior family histories,
Founder mutations can significantly influence regional prevalence. Genetic drift and population isolation have contributed to higher disease frequencies in certain geographic areas.
Muscular Dystrophy Subtypes
Duchenne Muscular Dystrophy: DMD is the most common and severe childhood muscular dystrophy. It is caused by mutations in the DMD gene, which encodes dystrophin, a cytoskeletal protein that links the intracellular actin cytoskeleton to the extracellular matrix through the dystrophin–glycoprotein complex. Absence of dystrophin results in sarcolemmal fragility and repeated cycles of muscle fiber damage.
DMD typically presents between ages 2 and 5 with proximal muscle weakness, delayed motor milestones, frequent falls, and a characteristic Gowers’ maneuver (in which a child uses their hands to “climb up” their own thighs in standing up from the floor). Progressive weakness leads to loss of ambulation, usually by early adolescence. Cardiomyopathy and respiratory insufficiency are the major causes of morbidity and mortality.
DMD is inherited in an X-linked recessive pattern, primarily affecting males, but female carriers may exhibit mild symptoms such as muscle weakness or cardiomyopathy due to skewed X-chromosome inactivation. While DMD, BMD, and female carriers have classically been thought of as separate disorders, the field has moved towards discussing all three as a spectrum of dystrophinopathy. This is partially because of significant phenotypic overlap (i.e. carriers can have a phenotype similar to DMD while patients with DMD mutations can have milder courses).
Roughly one-third of cases arise from de novo mutations, reflecting the large size and mutational susceptibility of the DMD gene.
Recently, Duchenne muscular dystrophy was added to the Recommended Uniform Screening Panel. While this panel is a recommendation only, many states have added DMD to their newborn screening panels, which will shift diagnosis earlier and allow for more aggressive use of novel therapies.
Myotonic Dystrophy: This is the most common muscular dystrophy in adults. It is distinguished by myotonia (delayed muscle relaxation) in addition to muscle weakness.
Two main types exist:
- Type 1 (DM1), caused by CTG repeat expansion in the DMPK gene
- Type 2 (DM2), caused by CCTG repeat expansion in the CNBP gene
These disorders are multisystemic, involving cardiac conduction defects, endocrine dysfunction, cataracts, and cognitive impairment.
Limb-Girdle Muscular Dystrophies (LGMD): LGMDs are genetically diverse disorders that affect the shoulder and pelvic girdle muscles. Many genetic subtypes have been identified, involving proteins such as sarcoglycans, dysferlin, calpain-3, and lamin A/C. Inheritance may be autosomal dominant or recessive, and disease onset ranges from childhood to adulthood.
Becker Muscular Dystrophy: BMD is one of the most common adult-onset MDs; it results from partially dysfunctional dystrophin and typically has a milder phenotype, with onset in adolescence or later, and slower progression.
Congenital Muscular Dystrophies: Babies with these forms of MD present with hypotonia, muscle weakness, and delayed motor development at birth or early infancy. Many subtypes involve defects in extracellular matrix proteins such as laminin-α2 (merosin) or proteins related to glycosylation of α-dystroglycan.
Facioscapulohumeral Muscular Dystrophy: FSHD is characterized by weakness affecting the facial muscles, scapular stabilizers, and upper arms. It is usually inherited in an autosomal dominant pattern and is associated with aberrant expression of the DUX4 gene due to contraction of the D4Z4 repeat region on chromosome 4. Disease progression is typically slow, but variable.
Emery–Dreifuss Muscular Dystrophy (EDMD): EDMD is characterized by early joint contractures, slowly progressive muscle weakness (typically affecting the shoulders, upper arms, and calves), and significant cardiac involvement.
It can be caused by mutations in several genes, most commonly EMD (X-linked) or LMNA (autosomal dominant). A defining feature is early cardiac conduction disease, which can lead to arrhythmias and sudden cardiac death.
Oculopharyngeal Muscular Dystrophy: This dystrophy is a late-onset disorder characterized by progressive ptosis and dysphagia, typically beginning in mid-to-late adulthood. It is most commonly caused by a GCN codon repeat expansion in the PABPN1 gene and may lead to proximal limb weakness over time.
Distal Muscular Dystrophy: This heterogeneous group of disorders is characterized by progressive weakness predominantly affecting the distal muscles of the hands and feet. Onset and severity vary widely by subtype, with some forms presenting in early adulthood and others later in life.
Incidence and Prevalence
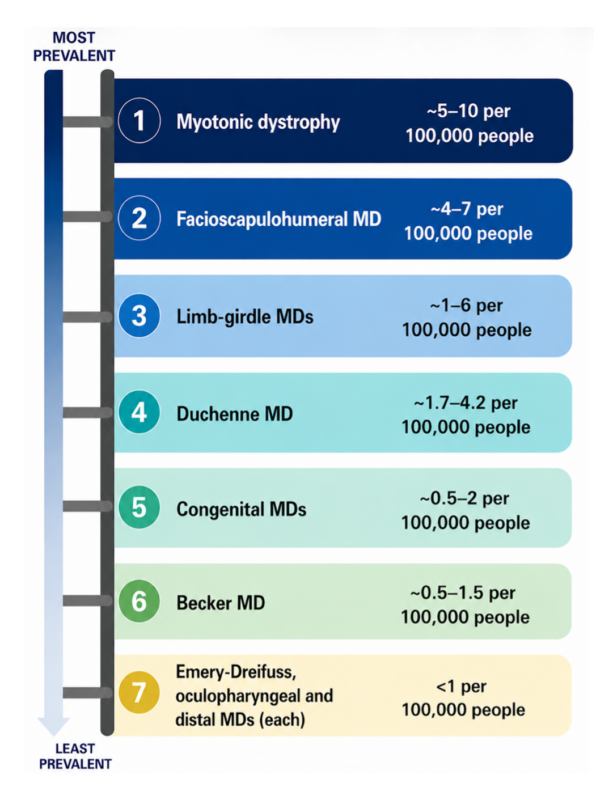
Although muscular dystrophies are individually rare, their combined prevalence represents a substantial burden of inherited neuromuscular disease. Epidemiologic data vary by region due to differences in genetic backgrounds, diagnostic practices, and availability of genetic testing.
US Prevalence of Muscular Dystrophy
The incidence of DMD in the U.S. has remained stable at approximately 1 in 3,500 to 5,000 live male births, while prevalence is increasing with improved survival. Today, this is estimated at ~2.8 per 10,000 males.
The overall prevalence of all muscular dystrophies combined is estimated to range from approximately 15 to 30 per 100,000 individuals worldwide. Population-based studies in North America and Europe report similar prevalence rates, although certain subtypes demonstrate geographic variation.
Improved genetic diagnostics over the past two decades have led to increased detection and more accurate subtype classification, influencing reported prevalence.
Public Health Impact
Although rare individually, muscular dystrophies collectively impose substantial healthcare and societal burdens due to their chronic and progressive nature, requiring multiple supports to optimize survival and quality of life.
Patients often require multidisciplinary care involving neurology, cardiology, pulmonology, orthopedics, rehabilitation medicine, and genetic counseling.
Improved survival in conditions such as DMD—due to corticosteroid therapy, cardioprotective medications, and advances in respiratory care—has increased the number of adults living with these disorders.
Advances in molecular genetics have substantially improved diagnostic precision and understanding of epidemiology. Recent treatment developments, including exon-skipping therapies, gene replacement strategies, and RNA-targeted treatments, are transforming the therapeutic landscape and augur higher survival prospects.
Clinical management of DMD, in particular, is benefitting from therapies derived from specific DMD research— especially those that aim to protect the vulnerable heart and cardiovascular system—as well as from broader research in neuromuscular disorders.
References
- Global epidemiology of Duchenne muscular dystrophy: An updated systematic review and meta-analysis. Crisafulli, S., et al. (2020). Orphanet Journal of Rare Diseases, 15(1), 141.
- Duchenne muscular dystrophy. Duan, D., et al. (2021). Nature Reviews Disease Primers, 7(1), 13.
- The DMD gene and therapeutic approaches to restore dystrophin. Fortunato, F., Farnè, M., & Ferlini, A. (2021). Neuromuscular Disorders, 31(10), 1013–1020.
- A review of muscular dystrophies. Hoang, T., & Dowdy, R. A. E. (2024). Anesthesia Progress, 71(1), 44–52.
- A systematic review and meta-analysis on the epidemiology of Duchenne and Becker muscular dystrophy. Mah, J. K., et al. (2014). Neuromuscular Disorders, 24(6), 482–491.
- A systematic review and meta-analysis on the epidemiology of the muscular dystrophies. Mah, J. K., et al. (2016). Canadian Journal of Neurological Sciences, 43(1), 163–177.
- Females with X-linked muscle disorders: An underestimated patient population. Politano, L. (2025). Acta Myologica, 44(1), 33–36.
- Global prevalence of Duchenne and Becker muscular dystrophy: A systematic review and meta-analysis. Salari, N., et al. (2022). Journal of Orthopaedic Surgery and Research, 17(1), 96.
- Prevalence of muscular dystrophies: A systematic literature review. Theadom, A., et al. (2014). Neuroepidemiology, 43(3–4), 259–268.
- Facioscapulohumeral muscular dystrophy and DUX4: Breaking the silence. van der Maarel, S. M., Tawil, R., & Tapscott, S. J. (2011). Trends in Molecular Medicine, 17(5), 252–258.
- A retrospective cohort study and review of the literature about germline mosaicism in Duchenne/Becker muscular dystrophy prenatal counseling: How to estimate the recurrence risk in clinical settings? Verebi, C., et al. (2025). Journal of Genetic Counseling, 34(1), e1932.
- The muscular dystrophies. Wicklund, M. P. (2013). Continuum (Minneapolis, Minn.), 19(6 Muscle Disease), 1535–1570.