
 Discussion
Discussion
Types of muscular dystrophy
Last updated Aug. 29, 2025, by Lindsey Shapiro, PhD
 Fact-checked by Jose Lopes, PhD
Fact-checked by Jose Lopes, PhD
Muscular dystrophy (MD) is a group of genetic muscle disorders that cause progressive muscle weakness and degeneration. There are more than 30 types, each with different genetic causes and symptoms. While the most common MD types appear during childhood, other forms affect adults only.
A key part of reaching an MD diagnosis is to accurately identify its type. The progression of MD symptoms, treatment approaches, and long-term outlook can vary significantly between different forms of MD.
Classification of muscular dystrophy
All MD types are caused by genetic mutations that impair the production or function of proteins important for muscle health, leading to progressive muscle weakness.
Despite these commonalities, it is key to know the specific disease type because it helps doctors understand the expected MD symptoms and their progression, as well as the necessary MD treatment approach in each individual case.
At the time of diagnosis, doctors will likely run a number of different tests to determine the specific type of MD a person has. This classification is based on:
- the underlying genetic cause of the disease
- disease severity and progression rate
- pattern of affected muscles
- age of onset.
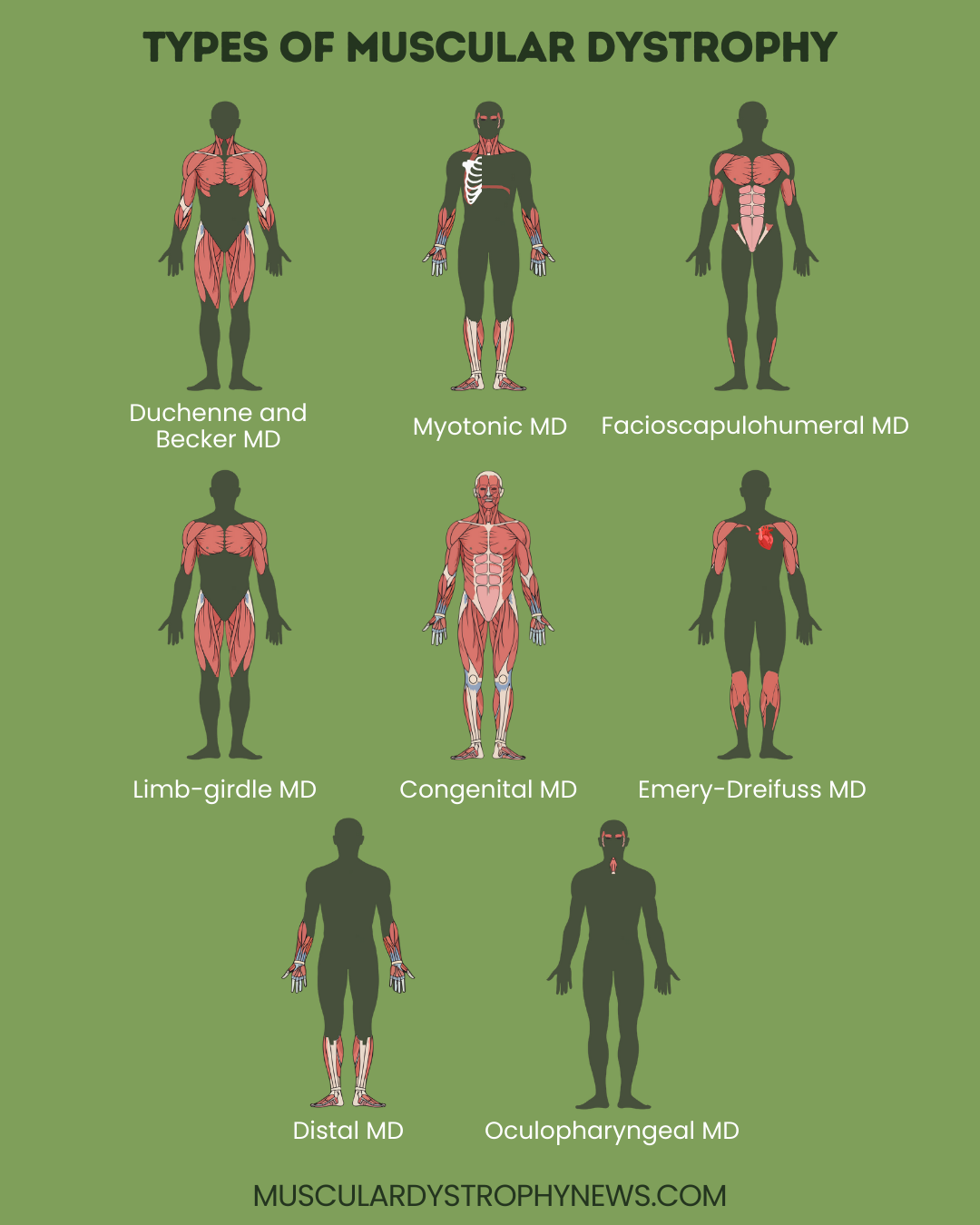
Major types of muscular dystrophy
There are many types of muscular dystrophy, which can be broadly grouped into nine main categories based on their typical presentation and underlying genetic MD causes:
Duchenne muscular dystrophy (DMD)
Duchenne muscular dystrophy (DMD) is the most common type of MD. It is caused by mutations in the DMD gene, leading to a complete or near complete loss of the dystrophin protein. Because of the way it is inherited, DMD predominately affects males.
Muscle weakness is usually evident in early childhood, starting in the legs, thigh, shoulders and pelvis, then later affecting other muscle groups. DMD progresses quickly, and most people completely lose their ability to walk by early adolescence. Heart disease, breathing issues, and spinal deformities are also prominent.
DMD is typically treated with corticosteroids and/or disease-modifying therapies to slow muscle decline, along with other interventions for symptom relief. Life expectancy has improved in recent years due to advances in care and treatment.
Becker muscular dystrophy (BMD)
Becker muscular dystrophy (BMD), among the most common types of MD, is also caused by DMD gene mutations and occurs mostly in males.
BMD has similar symptoms to DMD, but is generally milder and progresses more slowly because dystrophin production is less affected. Symptoms emerge in adolescence or early adulthood, and may or may not necessitate a wheelchair in adulthood. Complications like scoliosis and heart disease are not as common as in DMD.
BMD treatment is focused on symptom management. People with BMD usually live well into adulthood, with many having a relatively normal life expectancy.
Myotonic dystrophy
Myotonic dystrophy is the most common form of adult-onset MD, and is caused by mutations in the DMPK (type 1) or CNBP (type 2) genes.
Muscle weakness is accompanied by the defining feature of myotonia, where muscles are unable to relax after a contraction. Most people experience their first symptoms around age 20 or 30, although it is possible for symptoms to appear in childhood or later in adulthood. Problems with the heart, breathing muscles, eyes, and digestive tract are also common.
Symptoms usually progress gradually, but life expectancy may be affected. Type 2 myotonic dystrophy is generally milder than type 1, and among people with type 1, earlier onset forms are more aggressive than adult-onset forms. Treatment is focused on symptom control.
Facioscapulohumeral muscular dystrophy (FSHD)
Facioscapulohumeral muscular dystrophy (FSHD) is caused by abnormalities in a section of DNA on chromosome 4 called the D4Z4 region. It usually affects muscles in the face, shoulders, and upper arms, although the lower legs and hips may also eventually be affected.
Age at onset is highly variable, but the disease most commonly emerges in adolescence, with the majority of patients experiencing symptoms by the time they are 20. FSHD generally progresses very slowly, and rarely leads to complications like heart and breathing problems. Life expectancy is typically normal. Treatment involves supportive care and symptom management.
Limb-girdle muscular dystrophy (LGMD)
Limb-girdle muscular dystrophy refers to a group of more than 20 muscular dystrophies characterized mainly by weakness and wasting in the muscles around the shoulders and hips due to mutations in one of several different genes. Age of onset ranges from early childhood to adulthood.
The disease’s severity varies substantially, with some people losing walking ability and experiencing severe disability within a few years, and others never experiencing more than minimal disability. The disease tends to progress more rapidly in those that have a childhood onset.
Management of LGMD involves supportive care to improve function in day-to-day life.
Congenital muscular dystrophy (CMD)
Congenital muscular dystrophy (CMD) refers to a large group of muscular dystrophies characterized by symptoms of general muscle weakness that are evident at birth or in infancy. Joint deformities, breathing and swallowing issues, vision problems, seizures and cognitive issues are also possible.
There are more than 30 subtypes of CMD, differing in terms of the the affected gene and clinical presentation. Some of the most well recognized include:
- LAMA2-related MD
- Bethlem myopathy
- Ullrich CMD
- Fukuyama CMD
- Muscle-eye-brain disease
- Rigid spine MD
- Walker-Warburg syndrome
The exact course of CMD varies, with some being slowly progressive and others causing a shortened lifespan. Treatment involves symptomatic and supportive care.
Emery-Dreifuss muscular dystrophy (EDMD)
Emery-Dreifuss muscular dystrophy (EDMD) usually emerges in childhood or adolescence, affecting the shoulders, upper arms, and shins. Joint stiffness and deformities are common, as are heart problems. EDMD most commonly affects boys.
This type of muscular dystrophy may be caused by mutations in the EMD, FHL1, or LMNA genes. EDMD progresses slowly, and muscle weakness may not cause disability until later in life, but eople with the disease often develop heart problems by age 30. Disease management involves managing joint and heart problems.
Distal muscular dystrophy
Distal muscular dystrophy encompasses a group of conditions primarily affecting the muscles farthest from the core of the body — the hands, forearms, lower legs, and feet. There are several types:
- Finnish (tibial)
- Welander
- Miyoshi
- Nonaka
- Gowers-Laing
- distal myopathy with vocal cord and pharyngeal weakness
- hereditary inclusion-body myositis type 1
- VCP myopathy
Many different genetic defects cause the various subtypes of distal MD, which have distinct clinical profiles. Distal MD typically emerges in middle adulthood, although the exact age of onset varies by disease subtype. It generally progresses slowly, rarely leads to complete disability, and does not usually affect life expectancy.
Oculopharyngeal muscular dystrophy (OPMD)
Oculopharyngeal muscular dystrophy (OPMD), a rare type of MD, is characterized mainly by weakening in the muscles that control the eyes and the throat. Symptoms usually appear when a person in their 40s or 50s, with the first symptoms typically being difficulty swallowing and drooping eyelids. As the disease progresses, patients may have weakening in muscles elsewhere in the body, which can impact mobility.
OPMD progresses slowly and generally does not affect life expectancy. Treatment involves surgeries or other interventions to ease symptoms.
Muscular Dystrophy News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion